Life after cancer treatment is different. So are the health needs.
Nearly 10 years after Kara Kenan of North Carolina finished treatment for advanced breast cancer, her routine bloodwork revealed an increased level of an enzyme called alkaline phosphatase. KenanŌĆÖs primary care doctor didnŌĆÖt think that was important, so he ordered no further tests.
But Kenan, who directs marketing for the advocacy group Cancer Nation, knew better: That anomalous blood test could have been a sign that her cancer had spread to other tissues. She contacted her oncologist, who immediately ordered a computerized tomography (CT) scan. ŌĆ£And the CT revealed I had lesions on my liver,ŌĆØ she tells .
Kenan is one of about ŌĆö thatŌĆÖs more than 5% of the population. Almost all those patients need ongoing care, known as survivorship care, from clinicians who know the details of their cancer, their treatment, and potential problems that can show up decades later. But most do not receive this care, in part because of a longstanding communication gap between the oncologists who treat cancer and other clinicians who take care of the patient.
Instead, many must fend for themselves, often unaware of the cancer-related health risks that should be monitored. ŌĆ£We support patients really well during treatment and provide lots of resources,ŌĆØ says Michelle Mollica, director of survivorship care delivery at Hollings Cancer Center in Charleston, South Carolina. ŌĆ£And then we sort of graduate them, they ring a bell, and we expect them to go on after their cancer treatment is over, like their life is back to normal, but itŌĆÖs not.ŌĆØ
Advocates are not giving up on their conviction that survivorship care plans ŌĆö an idea proposed 20 years ago ŌĆö can solve the problem.
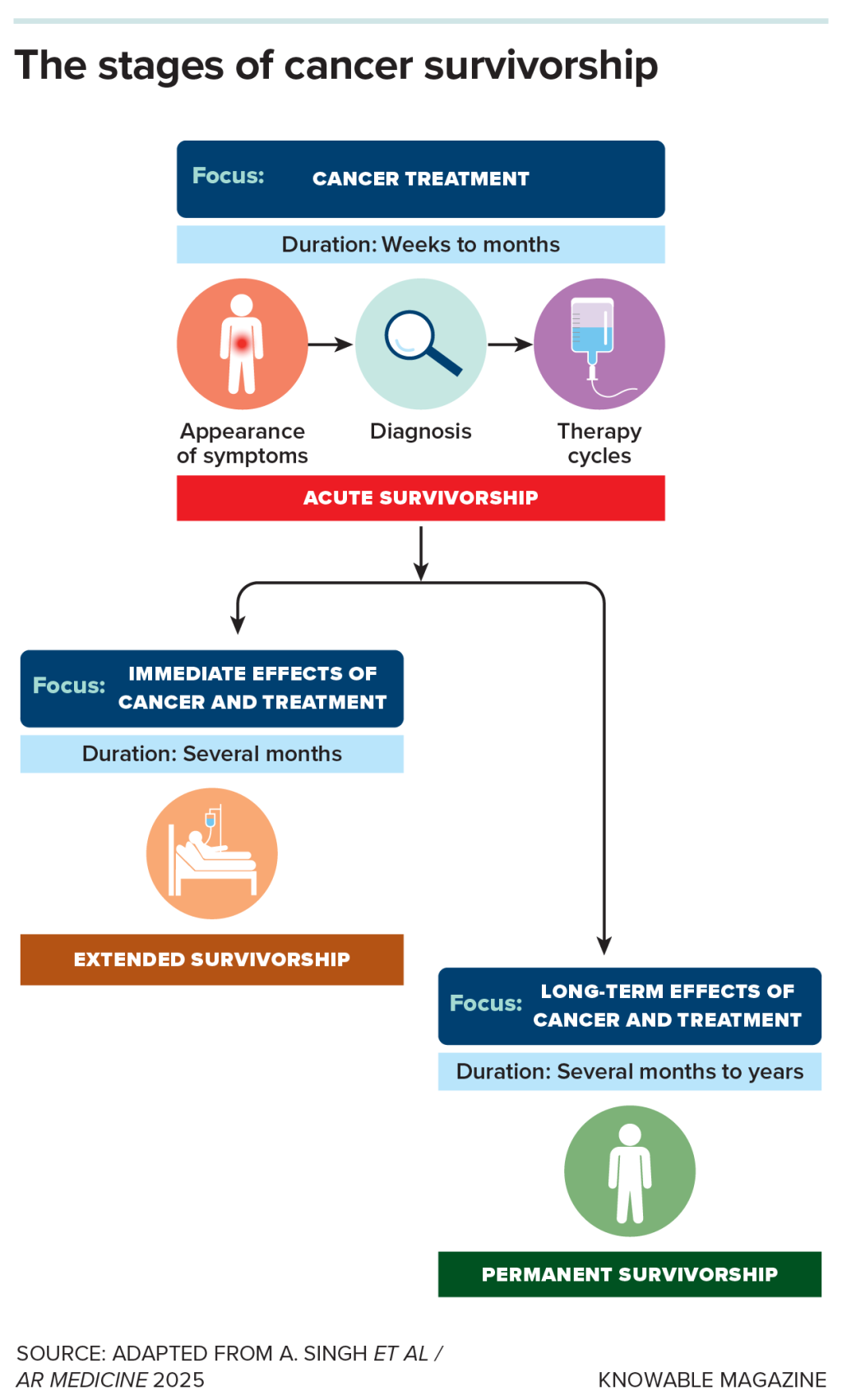
Long-term risks
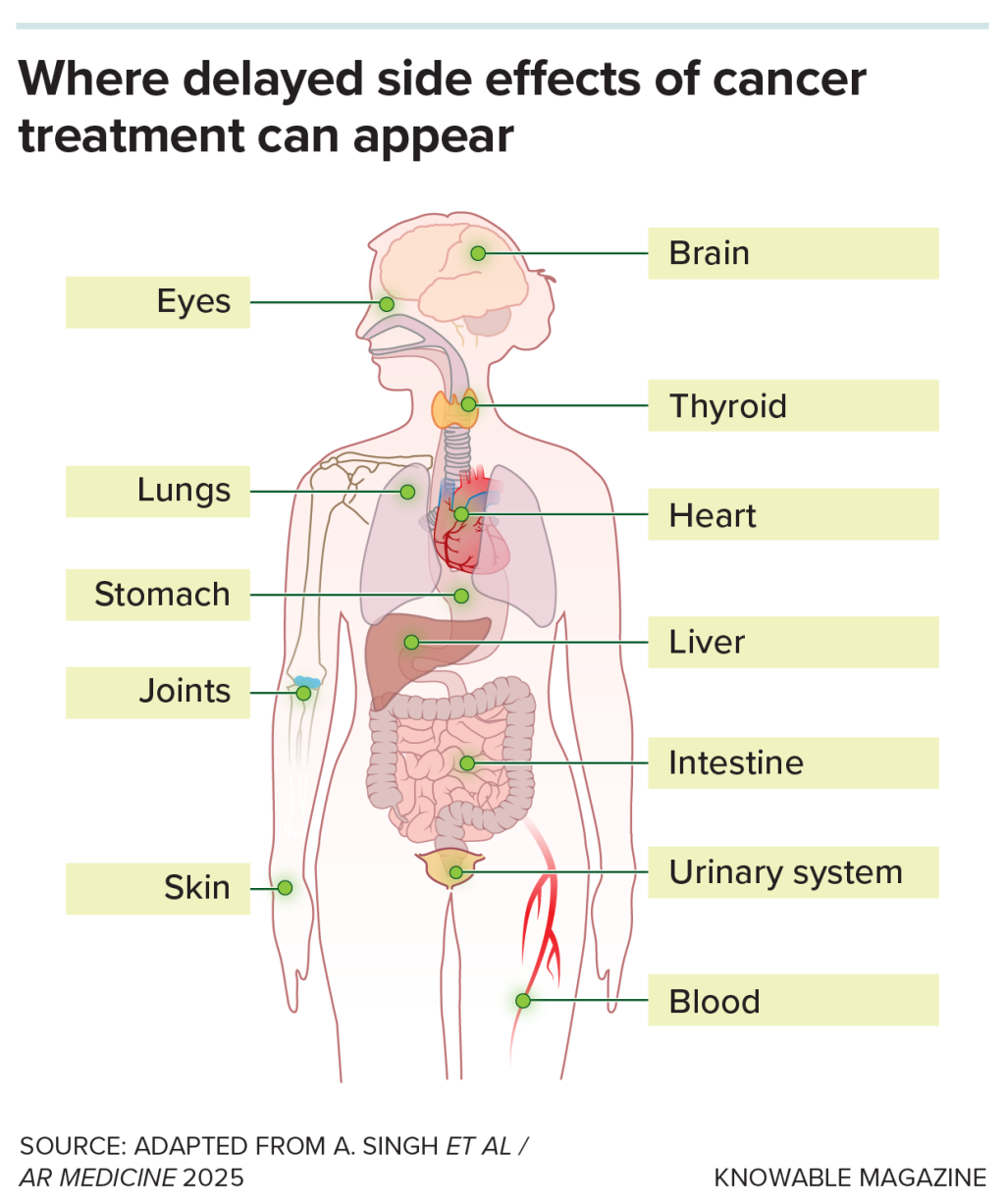
Treatment for cancer leaves long-lasting marks on the body, accelerating and exacerbating existing health problems. Chemotherapy, radiation, and other treatments can damage a patientŌĆÖs immune, gastrointestinal, endocrine, and neurological systems, and are associated with pain and fatigue, sleep problems, money worries, sexual dysfunction, depression, anxiety, obesity, and more.
have a 47% higher rate of developing cardiovascular disease than people who never had cancer, for example, and they have higher rates of pain, insomnia, and psychosocial distress. Survivorship care includes identifying and managing these side effects, which can be long-lasting and difficult to treat.
The risk that a cancer might recur years after apparently successful treatment is, obviously, a concern for many patients, but survivors also have an increased risk of developing new cancers, even decades later. ŌĆ£If we look at the 2 million people diagnosed with cancer each year, about 20% are people who are having second or third cancers,ŌĆØ says Patricia Ganz, associate director for population science research at the UCLA Health Jonsson Comprehensive Cancer Center.
The need for comprehensive survivorship care to address these ongoing issues has been recognized for decades: The National Coalition for Cancer Survivorship (now ) was started in 1986, and the National Cancer InstituteŌĆÖs Office of Cancer Survivorship followed a decade later. A 2006 report from the Institute of Medicine (now the National Academy of Medicine), , also flagged the problem. Nonetheless, a systematic way to provide that care to those who need it has never been developed.
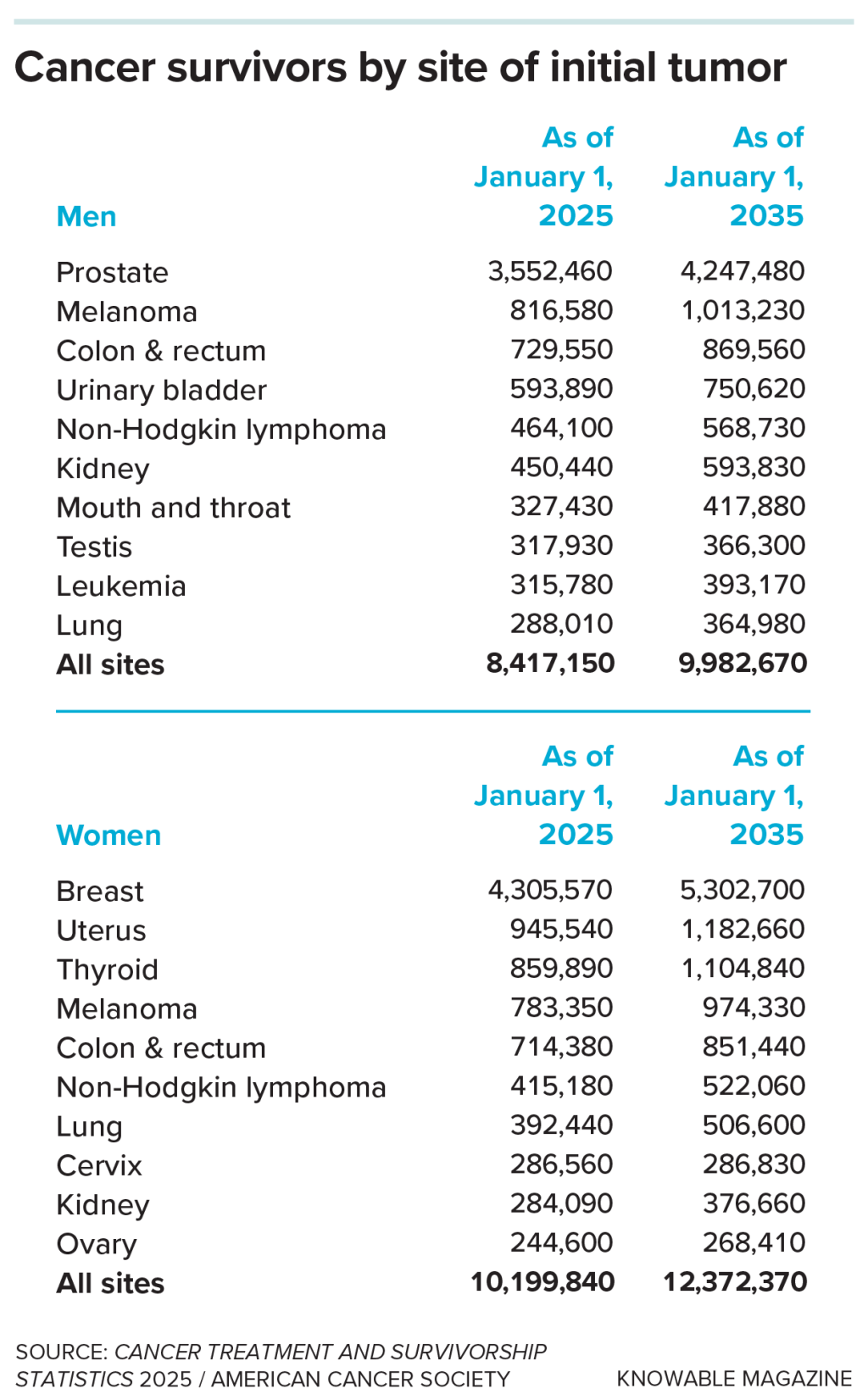
The need for such a solution is growing because the number of survivors is increasing rapidly as improvements in detection and treatments mean more cancer patients are living long lives after diagnosis. In 1971, an estimated 3 million Americans were cancer survivors; by 2035, that number is expected to surpass .
Yet only about a third of people who completed treatment five years earlier or longer , according to a 2025 survey of patients undergoing cancer treatment and survivors. Of all patients no longer receiving post-treatment care, 58% reported that their doctor said it was no longer needed.
That may reflect the fact that, in general, neither oncologists nor other clinicians are well trained to provide long-term survivorship care, Ganz says. She served on the Institute of Medicine committee that produced the Lost in Transition report. ŌĆ£It was really championed by people who were cancer survivors who said, ŌĆśLook, when I go to my family doctor, they say, ŌĆśOh, I donŌĆÖt know anything about that. Go back to your oncologist,ŌĆÖŌĆØ she says.
But this isnŌĆÖt ideal, says Alex Adjei, chief of Cleveland ClinicŌĆÖs Cancer Institute and coauthor of an in the 2025 Annual Review of Medicine: After a patientŌĆÖs cancer is successfully treated, the patient should be handed off to other clinicians who are trained to address their hypertension, diabetes, and other health problems. ŌĆ£If you donŌĆÖt do that,ŌĆØ he says, ŌĆ£itŌĆÖs a disservice.ŌĆØ
Shared responsibility
The National Cancer Institute says the best approach is for primary care providers and oncologists to . Primary care providers should manage a patientŌĆÖs chronic conditions like diabetes and high blood pressure, screen for other cancers, and encourage healthy habits such as weight management, while oncologists focus on cancer recurrence, says Mollica, who was deputy director of the National Cancer InstituteŌĆÖs Office of Cancer Survivorship until 2025. But though patients may indeed see more than one doctor, that type of collaboration is not common. ŌĆ£ThereŌĆÖs often issues with coordination and communication, so lots of fragmented care,ŌĆØ she says.
The Institute of MedicineŌĆÖs report sought to overcome that problem two decades ago. Its recommendation: When cancer treatment ends, the patient and their primary care physician should receive from the cancer doctor a that details what to expect during recovery, what ongoing care is needed (mental health services to treat depression or physical therapy to help with mobility, for example), and the schedule for recommended cancer screening and other tests. For a few years, the Commission on Cancer, the accreditation body for cancer programs, even required survivorship care plans.
But , for several reasons. By the time a patientŌĆÖs treatment ends, their medical record contains months and even years of test results, tumor characteristics, surgeries, and other therapies, and other information that might inform their health for the rest of their lives. ThatŌĆÖs a lot of information to convey, without an easy way to convey it.
Oncologists balked at the unpaid work involved in compiling all that information and didnŌĆÖt fully commit to the effort. ŌĆ£It was like, hereŌĆÖs a piece of paper, this is going to change your care, and it just didnŌĆÖt,ŌĆØ Mollica says. ŌĆ£It became a checkbox, and not a conversation and ongoing process for survivorship care.ŌĆØ Possibly because few patients actually received plans ŌĆö and, in some cases, neither patient nor primary care physician knew what to do with them ŌĆö .
Some large cancer centers have successfully applied the care-plan model, though. At the Cleveland Clinic, Adjei is working to create a system in which all survivors get the care appropriate for their specific situations.
For example, adolescents and young adults are treated at the Integrated Program for Young People with Cancer, which can address their special needs, such as strategies to balance cancer treatment with fertility preservation. Another clinic identifies survivors with genetic damage from cancer therapy that affects bone marrow and, over many years, increases an individualŌĆÖs risk of heart disease and blood cancers. And survivors who received relatively novel therapies, for which long-term effects are still uncertain, are treated at the Cleveland ClinicŌĆÖs Oncology Pharmacovigilance Clinic, where rheumatologists, dermatologists, psychiatrists, pulmonologists, and other specialists monitor side effects.
But most patients who go to the Cleveland Clinic for cancer treatment get their survivorship care from the oncologist who treated their cancer. And many of them want to continue seeing their oncologist. ŌĆ£This is like a psychological crutch for them, and thereŌĆÖs separation anxiety,ŌĆØ Adjei says. But Adjei thinks closer collaboration with primary care would benefit everyone. Men who have had prostate removal after a cancer diagnosis do not necessarily need a cancer specialist to monitor for markers of recurrence. ŌĆ£They could easily go to their primary care so that their urologists can have time to deal with the surgeries they need to do,ŌĆØ he says.
And so Adjei and colleagues are currently working to assemble a range of services ŌĆö mental health, social work, financial counseling, and others ŌĆö that survivors frequently need. ŌĆ£And my end goal is to integrate our primary care group into it,ŌĆØ he says.
Despite these promising efforts at the Cleveland Clinic and other major centers, the nationwide story on survivorship care plans is not good. Only 36% of cancer patients who complete treatment receive such a plan, according to the 2025 survey of survivors. To improve that record, Cancer Nation, the advocacy organization, is pushing Congress to pass the and , which would require Medicare to pay health care providers for creating survivorship plans and coordinating with other clinicians to make sure survivors get the care they need.
Until that happens, many cancer survivors will be left on their own. In KenanŌĆÖs case, the lesions on her liver turned out to be benign. But the fact that her primary care physician did not know the significance of rising levels of alkaline phosphatase in her blood reflects inadequate communication and coordination that risks a survivorŌĆÖs health. ŌĆ£ThatŌĆÖs a real problem,ŌĆØ she says.
Survivorship plans could solve many issues, providing detailed information to facilitate conversations, easing the burden on primary care providers, and relieving survivors of stress and worry. The result, she says, is that ŌĆ£we all get better care.ŌĆØ
was produced by and reviewed and distributed by ▒¼┴ŽTV.